
The MRI can say more than a standard read
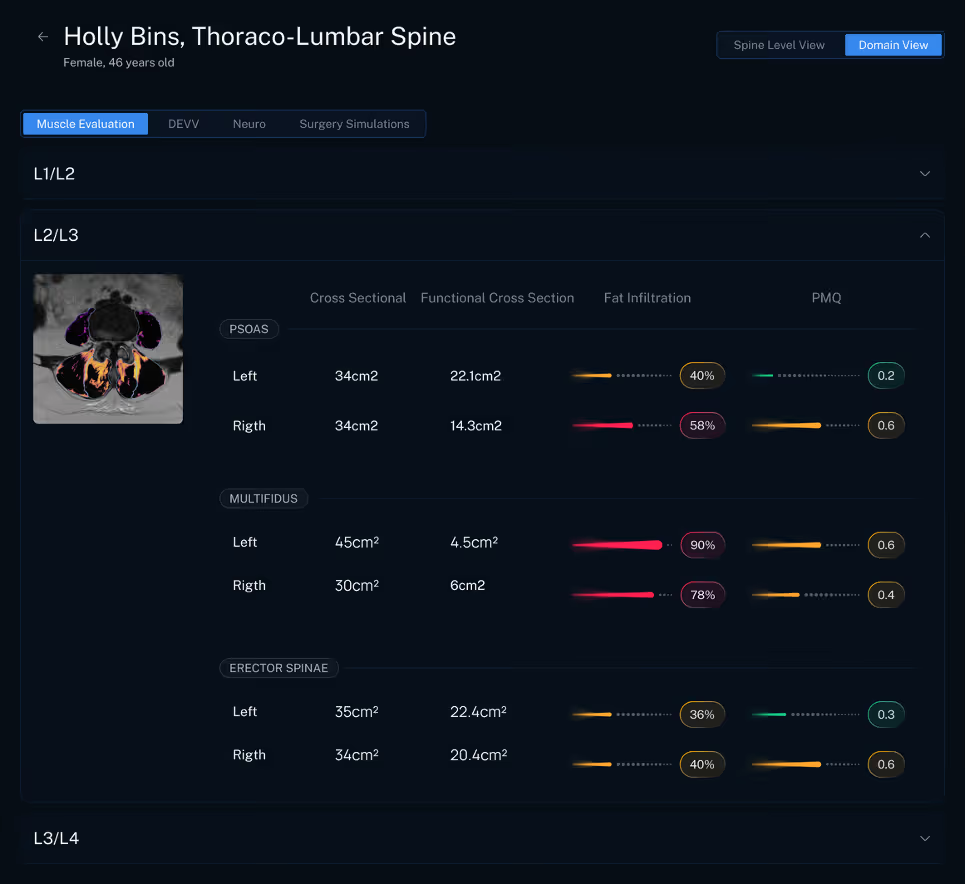
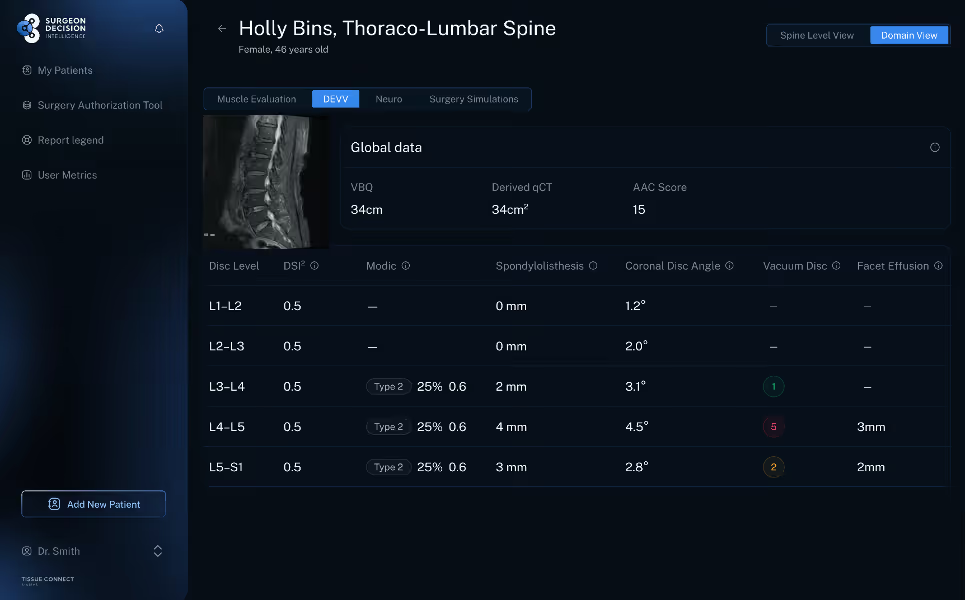
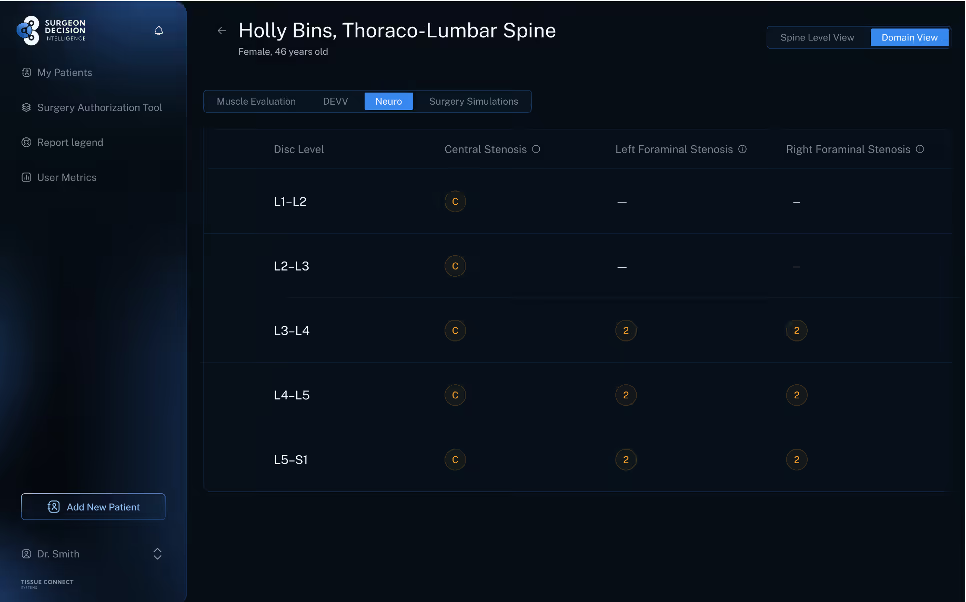
Most spine surgery planning still begins with a familiar routine. A surgeon reviews the MRI, matches the imaging to the patient’s symptoms, and decides what surgery the patient may need. That process works, but it often leaves important information on the table. A standard read may describe stenosis, disc degeneration, and alignment, yet it may not fully describe the tissue environment that will support, or undermine, the operation. The Tissue Typing module in the SurgeonDecision Intelligence Platform is built to close that gap. It extracts level by level quantitative imaging biomarkers, or QIBs, from each spine MRI. Those biomarkers include muscle metrics such as functional cross sectional area, fat infiltration percentage, fibrous intrusion, and paraspinal muscle quality score. They also include disc and endplate metrics such as the DSI squared score and Modic related change, bone quality metrics such as VBQ and MRI derived QCT, and neuro and facet findings such as central stenosis, foraminal stenosis, and facet joint effusion size.
Why that matters in the operating room
Two patients can both carry the label of lumbar stenosis and still present very different surgical problems. One may have strong paraspinal muscle, preserved disc biology, and solid bone. Another may have severe multifidus degeneration, endplate change, poor bone quality, and signs of segmental instability. Those differences can influence whether decompression alone is likely to hold up, whether a fusion should be considered earlier, whether a muscle sparing approach makes more sense, and whether the implants should prioritize broader endplate support. In that sense, QIBs are not just descriptive numbers. They can guide strategy.They can help surgeons match technique, modality, and construct choice to the actual tissue in front of them rather than to diagnosis alone [4][5][6].
Muscle quality may be the most underused planning signal
The strongest opportunity may be in the paraspinal muscles. Several studies summarized in your research packet show that poor muscle quality is associated with harder postoperative courses and less durable results. Higher posterior paraspinal fatty infiltration has been linked to earlier conversion from decompression to fusion after lumbar laminectomy. Multifidus fatty infiltration has also been identified as the strongest MRI based predictor of revision for adjacent segment disease after posterior lumbar fusion. In separate outcome studies, higher erector spinae fatty infiltration predicted worse disability two years after surgery, while multifidus degeneration showed a more specific relationship with walking and standing function [4][5][7].
That matters because muscle quality can shape the surgical plan before the first incision. If the MRI shows severe multifidus damage, low functional cross sectional area, and substantial fat or fibrous replacement, many surgeons will want to preserve as much remaining muscle as possible. That may favor a less disruptive posterior exposure, a tubular decompression, an endoscopic approach, or another minimally invasive strategy when the pathology allows it. For a patient who still needs fusion, the same findings may argue against long open posterior dissection if a muscle sparing route can accomplish the same goal. The point is not that one approach is always best. The point is that tissue quality can and should influence how the operation is delivered [4][5][8].
The newer paraspinal muscle quality score adds another layer. Early evidence suggests that this score captures changes in lean muscle quality that standard area and fat measurements do not fully explain, and that it is associated with pain intensity. That makes it appealing as a practical summary metric. Instead of relying on one dimension of degeneration, surgeons can review a more complete picture of muscle reserve and mechanical support [1].
Disc and endplate biology can sharpen the fusion discussion
Disc degeneration is often described in broad categories, but quantitative disc biomarkers can make the conversation more precise. The DSI squared score offers an objective way to measure disc signal loss and degeneration on MRI. Research suggests that DSI squared captures clinically relevant degeneration patterns and can reveal nuance that traditional qualitative grading may miss [2][9].
When those disc findings are combined with Modic related change, the planning value increases. Modic changes, especially more advanced patterns, have been associated with worse long term outcomes after decompression, more residual pain, and higher risk of mechanical problems in some fusion settings. That does not mean every patient with Modic change needs a fusion. It does mean that a level with severe disc signal loss, endplate disruption, and Modic intrusion may deserve a different conversation than a level with compression alone. In some patients, these findings strengthen the case for stabilization rather than decompression only.In others, they support choosing an interbody strategy that restores height shares load better, and protects the endplates more effectively [6][9][10].
This is where surgical modality becomes practical. A biologically weak disc and endplate complex may make a wider footprint implant more attractive. That can support consideration of an ALIF or, in the right anatomy, a standalone lateral fusion. The value ofTissue Typing is that it helps make that reasoning explicit instead of intuitive. The disc is no longer just dark on T2. It becomes a quantified structure with a measurable risk profile [2][6][10].
Bone quality still changes everything
Bone quality is already a familiar driver of surgical planning, but it is often under measured in routineMRI based workups. VBQ and MRI derived QCT can help bring it into the same preoperative framework as muscle and disc quality. In published studies, higher VBQ scores have been associated with pedicle screw loosening, proximal junctional failure, and cage subsidence. VBQ has also shown meaningful correlation with QCT based bone density measures [3][11][12].
For surgeons, the implications are immediate. Poor bone quality may favor broader endplate contact, supplemental fixation, cement augmentation, or different implant geometry. It may also strengthen the argument for an anterior column strategy when endplate support is central to the construct. Bone quality is not a side note. It can change the entire mechanics of the plan [3][11][12].
Neuro and facet metrics help define when decompression may not be enough
The neuro metrics in Tissue Typing add context that standard narrative reports may blur. Foraminal stenosis has been associated with multifidus atrophy in a level specific pattern, which suggests that nerve compression and muscle degeneration often travel together. Cervical central stenosis has also been linked to fatty degeneration below the compressed level. These relationships can help explain why some patients appear functionally worse than the headline MRI finding woulds suggest [13][14].
Facet findings matter for the same reason. Facet joint effusion can be a clue to instability, and published work suggests that larger effusions or the combination of facet opening and effusion may identify patients at higher risk of failure after decompression alone. When a level shows severe stenosis, advanced disc degeneration, and meaningful facet fluid, the discussion may shift toward adding stabilization rather than relying on a limited decompression to solve a broader mechanical problem [15][16].
QIBs do not replace surgical judgment. They make surgical judgment more specific. They help surgeons move beyond broad labels and see the actual biology of the operative level. Muscle quality can support tissue preserving approaches. Disc and endplate biomarkers can sharpen the choice between decompression alone and stabilization. Bone quality can inform implant strategy. Neuro and facet metrics can highlight when compression is part of a larger instability problem. That is the real value of the Tissue Typing module. It turns the preoperativeMRI into a more useful map for choosing the right technique, the right modality, and the right approach for the patient in front of you.