
Why Two Year Outcomes Matter in Spine Surgery
In spine surgery, all follow-ups matter - the early follow up, the 90-day mark, the 1-year visit. But if we want a clearer picture of whether a surgery truly worked, the 2-year point often tells us much more. That is the point when many surgeons start to feel confident that an outcome is not just promising, but durable. It is also the point when patients begin to understand whether the operation changed their daily lives in a lasting way. Pain relief that holds for 2 years means more than a short burst of early improvement. Functional recovery that lasts for 2 years is more likely to reflect a real shift in the patient’s trajectory. In spinal degenerative disease, patient reported outcomes collected at 2 years correlate strongly with outcomes at 5 years. In adult spinal deformity surgery, improvements seen at 2 years tend to remain durable at longer follow up, even when small declines appear over time. That makes the 2 year mark a meaningful clinical checkpoint. [1][2]
The two year window also matters biologically. In fusion surgery, this period helps us judge whether the construct has truly consolidated. Bone healing begins much earlier, but by one to two years surgeons usually have a clear sense of whether the patient achieved a solid arthrodesis, whether there are hardware related issues, or whether adjacent segment pathology is emerging. The 2 year window also matters because it better reflects function in the real world. In a prospective cohort study of lumbar fusion patients, 76 percent returned to work within 24 months [3].
There is also a psychological dimension to the 2 year mark that is harder to quantify but very real to anyone who treats spine patients. By the time a patient reaches 2 years, they have invested enormously in their recovery. They have worked through the early pain, the physical therapy, the slow return to normal movement. They have started to feel like they got their life back. When a failure happens before or around that point, the emotional weight is significant. The patient is not just facing another procedure. They are facing the loss of a recovery they believed was behind them. Any surgeon who has sat across from a patient in that situation understands it. It shapes how we think about revision cases and why getting the first surgery right matters so deeply.
Ongoing and 2-year follow up gives surgeons a more honest picture of what the procedure achieved. This is exactly why we built the Surgical Simulations module of Surgeon Decision Intelligence.
2-Year Durability Indices
In the surgical simulation module, we predict and compare 2 year outcomes across surgical approaches before the case happens. That includes broad procedure categories that spine surgeons already consider every day, including arthroplasty, decompression, posterior fusion, lateral fusion, and anterior fusion. The point is not to replace judgment. The point is to strengthen it.
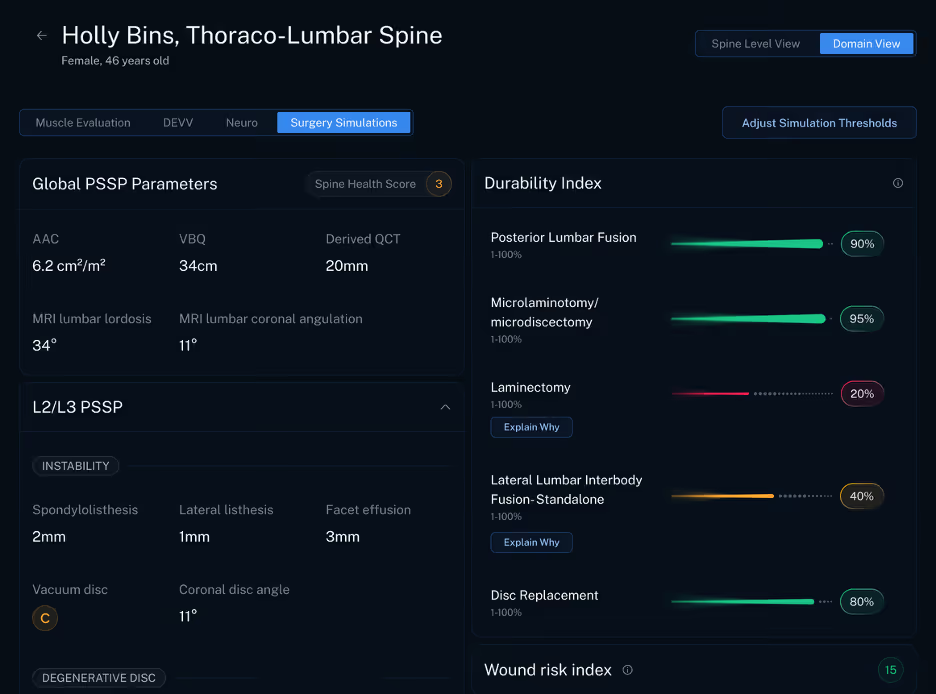
What makes this especially important is that our algorithm is implant agnostic. It does not begin with loyalty to one hardware system or one implant strategy. It focuses on the likely durability of the surgical approach itself. That matters because the best decision support tool should help surgeons think more clearly about the operation, not steer them toward a product preference. When a model stays implant agnostic, it has a better chance of giving surgeons a more balanced comparison across treatment paths.
That kind of comparison can be powerful in the clinic. It can help frame conversations that are often difficult, nuanced, and deeply personal. A surgeon can discuss not only what is technically feasible, but what is most likely to hold up over 2 years. That may help clarify when decompression alone is enough, when fusion offers a more durable answer, or when one corridor may offer advantages over another for a specific patient. It gives us more information to discuss with patients, and it can make approach selection more thoughtful and more transparent.
For hospital leaders, this matters too. Better procedural matching can improve consistency across service lines, support more disciplined use of resources, and reduce the cost of decisions that have to be revisited later. A tool that helps identify the right surgery earlier can improve more than an isolated case. It can improve the overall quality of decision making across a spine program.
This is the kind of answer many of us have hoped AI could bring to surgical care. Not just automation. Not just faster documentation. Real clinical support that helps us choose the right operation for the right patient. But durability is just the beginning.
Future Directions
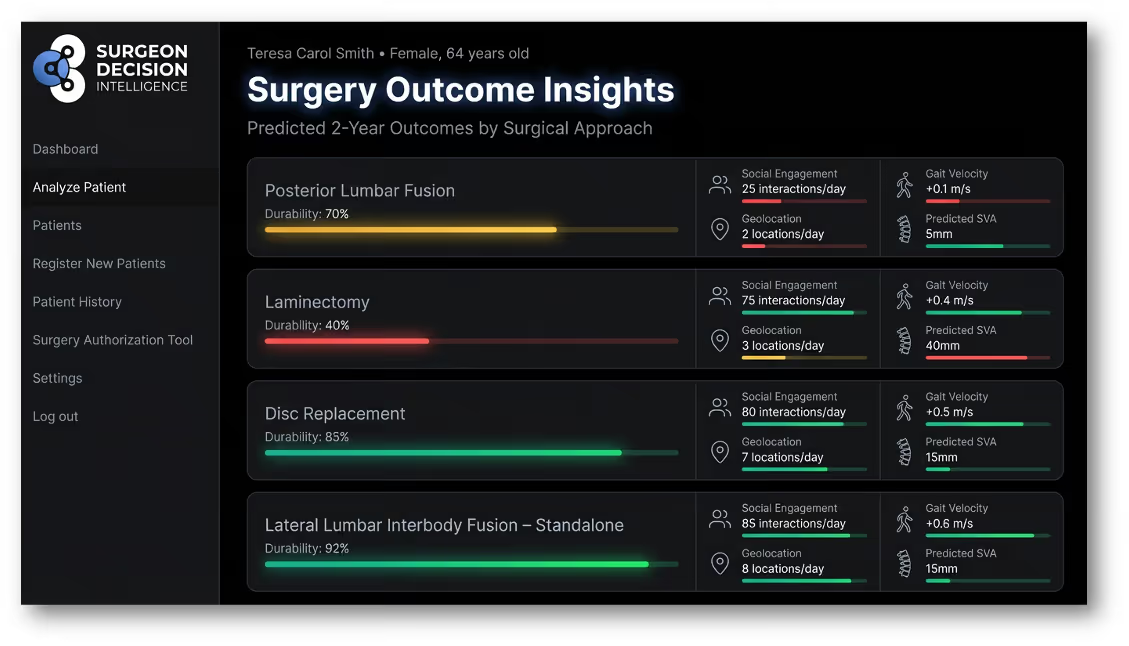
Our near term roadmap goes further. The next step is not only to predict whether a result will last, but to predict how a patient will function after surgery through digital outcome metrics. That means looking past traditional follow up measures and asking more detailed questions about lived recovery.
Can we predict improved posture? Can we estimate whether a patient is more likely to increase social engagement? Can we measure whether they begin visiting new places again instead of staying home? Can we identify likely gains in gait metrics that reflect confidence, mobility, and independence? These are not side issues. They speak directly to whether the patient is getting life back.
That level of prediction could reshape how we think about success in spine surgery. A patient may report less pain, but still remain largely home bound. Another patient may show only moderate change on a standard questionnaire, yet walk farther, stand taller, leave the house more often, and reconnect socially. Those differences matter. If we can predict them with greater granularity, we can plan surgery, counseling, recovery, and follow up in a much more patient centered way.
It could also improve shared decision making. Surgeons would be able to discuss not only which procedure is likely to be durable, but which one is more likely to improve the patient’s actual day to day function. That gives patients a clearer sense of what recovery may look like in real life, not just on paper.
For years, spine surgery has relied on a familiar group of outcome measures. We look at images, revision rates, complications, and patient reported scores. Those metrics still matter. But they do not fully capture how people move through the world after surgery. I believe the future of outcomes science lies in combining durability with digital function.
That is the vision behind Surgeon Decision Intelligence. Start with 2 year durability because it is one of the clearest windows into whether a procedure truly succeeded. Then build toward a model that predicts function with enough precision to make spine care more personal, more rigorous, and more useful to the people we treat.