Modic Changes: The “Peat Fire” Inside Vertebral Bodies That Can Shape Surgical Outcomes
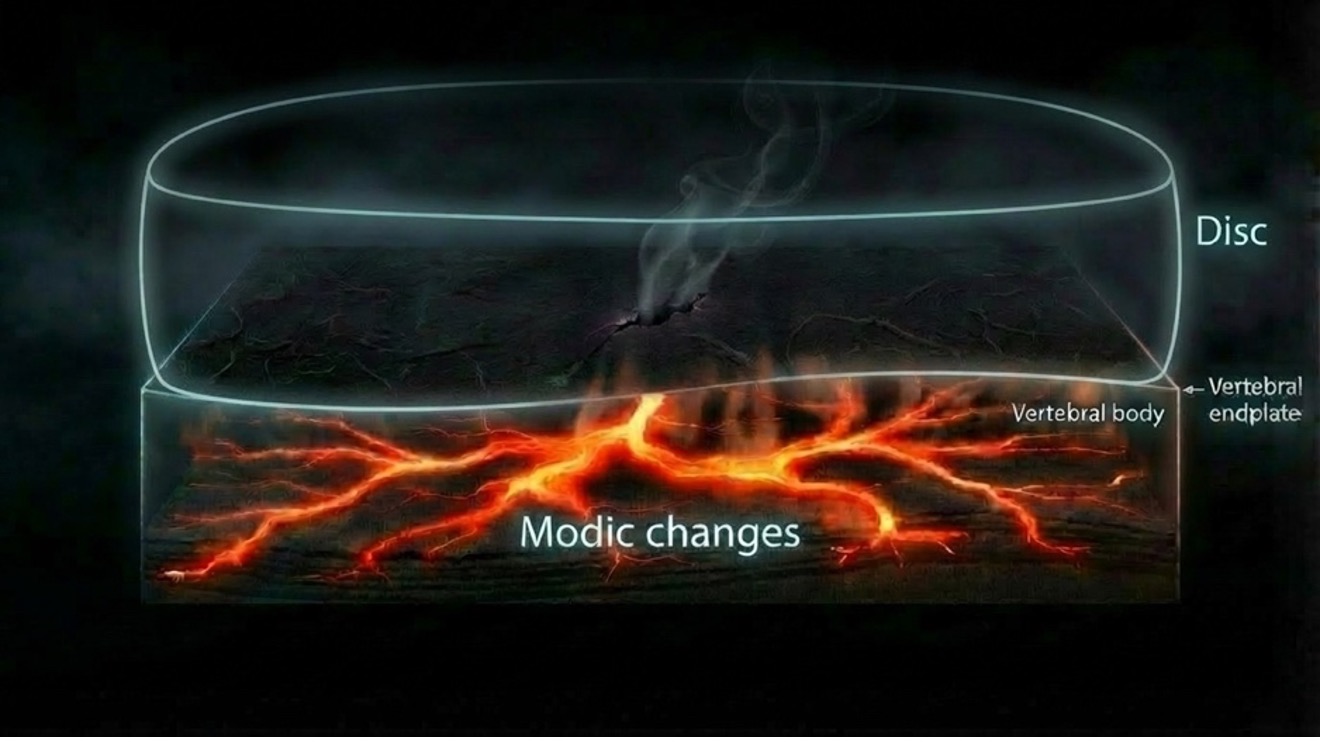
A peat fire can look like nothing is happening. The ground is dark. The air is still. There are no flames. But underneath, the soil is hot, and it keeps burning in slow motion. It spreads sideways through the peat, day after day, turning solid ground into weak, damaged ground. Even if you stamp out a small smoky spot on the surface, the fire can keep going below, because the real problem is not what you can see, it is the ongoing process underground.
That is a good way to think about Modic changes in the spine. A spinal level can look like “normal wear and tear” on the outside: some disc degeneration, some narrowing, maybe even a clear surgical target like stenosis. But Modic changes suggest something else is happening at that level in the vertebra: an active, irritated state, where inflammation and tissue remodeling keep the area sensitive. In other words, the segment is not just old and worn. It may still be smoldering [1–4]
And that matters because surgery often fixes the structure you can point to like taking pressure off a nerve or stabilizing a segment. But the biology in the bone can keep influencing the outcome. If the “peat fire” is still active at that level, the patient may have a higher risk of lingering pain, slower healing, or mechanical issues like poor early fusion or cage settling, depending on the procedure. The key idea is simple: Vertebral bone marrow lesions called Modic changes mark an active process at the disc-endplate-vertebra-junction which can determine surgical outcomes [5–11].
What are Modic changes?
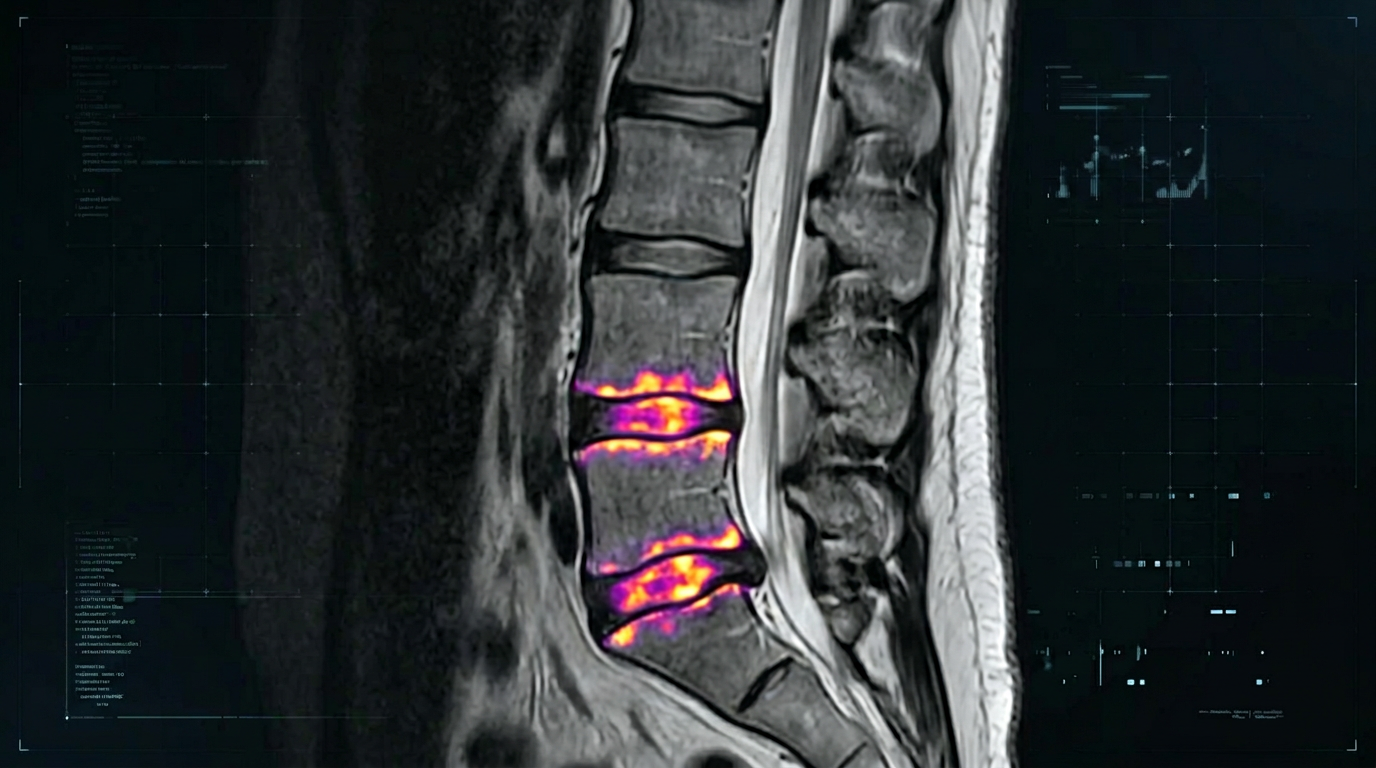
Modic changes are vertebral bone marrow lesions that appear on MRI right next to the vertebral endplates, the thin interface where the disc meets the vertebral body. In other words, they are abnormal MRI signal changes inside the vertebra usually above or below a degenerated disc at locations where the endplate is damaged[1,2].
What that really means is this: the endplate is like a thin “seal” between the disc and the bone. When that seal gets injured (e.g mechanically or even through bacterial products released from the disc), it can let the disc–endplate-bone marrow unit behave like a stressed, irritated interface [3].
The bone marrow behind the endplate is far more than simple “filler.” It harbors millions of immune cells that initially respond to structural damage or bacterial stimuli, but can subsequently drive tissue destruction, altered bone turnover, and nociceptive activation. This is why Modic changes represent more than a passive MRI finding: they reflect an active biological process within the vertebral bone [3,4,12,13].
Why are they called Modic changes? The explanation is straightforward: they are named after Dr. Michael T. Modic, the radiologist who, together with his colleagues, first described and classified these characteristic vertebral bone marrow signal patterns in the context of degenerative disc disease [1,2].
However, not all Modic changes are the same. Based on their appearance on two key MRI sequences—T1-weighted (T1w) and T2-weighted (T2w)—we distinguish three distinct Modic subtypes. Longitudinal studies suggest that these subtypes represent different stages along the same underlying pathological process.
The three classic Modic “types” (what MRI is showing)
On standard T1- and T2-weighted MRI, Modic changes are described in three main patterns:
- Type 1 (MC1): low signal (hypointense, dark) on T1w and high signal (hyperintense, bright) on T2w. This pattern is often treated as the most inflammatory and most painful phase, where the endplate region shows signs consistent with an irritated, reactive environment.
- Type 2 (MC2): high signal on both T1w and T2w images. This pattern reflects fatty marrow replacement near the endplate.
- Type 3 (MC3): low on both T1 and T2. This pattern is associated with a more sclerotic, scar-like bony state [3]
Why do we care about these Modic changes?
There are two reasons we care about this:
1) They contribute to pain
The endplate area has pain-sensitive nerve endings nearby. When the endplate is damaged and the adjacent marrow becomes inflamed and mechanically stressed, it can trigger pain through chemical and mechanical stimulation of nociceptors (tiny “danger sensors” at the ends of nerves that detect potential tissue harm and send a warning signal to your spinal cord/brain—your body’s pain alarm system) around that interface. That helps explain why Modic changes can be a strong clue to a painful level when they are present [3,14]
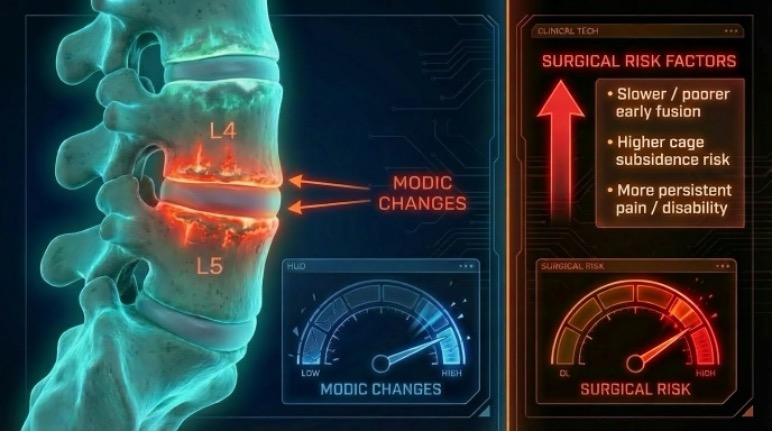
2) Their presence predicts surgical outcomes:
There is a large body of evidence that the presence of these Modic lesions influence surgical outcomes.
- Decompression for stenosis (10-year follow-up): If you have Modic Type 2 before surgery, you tend to have worse long-term recovery than people with Type 1 or no Modic changes [11]
- Stenosis surgery (2-year follow-up): If the Modic changes are large (take up a big part of the vertebra), patients end up with more back/leg pain and more disability after surgery—even if they started out similar before surgery [10]
- Transforaminal Lumbar Interbody Fusion (TLIF) fusion surgery: If Modic changes are present before surgery, the spine is less likely to fuse well, and the implant/endplate “bond” looks weaker on CT [9]
- Anterior Cervical Discectomy and Fusion (ACDF) (neck fusion): If Modic changes are present before surgery, fusion rates are a lower, and the cage is more likely to sink/settle (subsidence) [7]
- Overall takeaway from meta-analyses: Across studies, Modic changes are a warning sign for slower/poorer early fusion and a higher risk of cage subsidence, though the strength of the effect can vary by procedure [5,6]
Take home message
Modic changes are MRI-visible bone marrow lesions next to damaged endplates. They can act like a “smoldering hot spot” in a spinal segment. When Modic changes are present before surgery they can predict worse recovery, slower fusion, and higher implant settling (subsidence) risk.
References
[1] Modic MT, Steinberg PM, Ross JS, Masaryk TJ, Carter JR. Degenerative disk disease: Assessment of changes in vertebral body marrow with MR imaging. Radiology 1988;66:193–9. https://doi.org/10.1148/radiology.166.1.3336678.
[2] Modic MT, Masaryk TJ, Ross JS, Carter JR. Imaging of degenerative disk disease. Radiology 1988;168:177–86. https://doi.org/10.1148/radiology.168.1.3289089.
[3] Dudli S, Fields AJ, Samartzis D, Karppinen J, Lotz JC. Pathobiology of Modic changes. European Spine Journal 2016;25:3723–34. https://doi.org/10.1007/s00586-016-4459-7.
[4] Heggli I, Mengis T, Devan J, Herger N, Farshad M, Habib M, Ames CP, Distler O, Fields AJ, Dudli S. Modic Change Bone Marrow Neutrophils Are Activated and Degrade Cartilage Endplates. JOR Spine 2026;9. https://doi.org/10.1002/jsp2.70170.
[5] Duan Y, Feng D, Zhu M, Qiu H, Li T, Chen Z, Jiang L, Huang Y. Modic Changes Increase the Cage Subsidence Rate in Spinal Interbody Fusion Surgery: A Systematic Review and Network Meta-Analysis. World Neurosurg 2024;181:64–72. https://doi.org/10.1016/j.wneu.2023.10.080.
[6] Chen R, Zou K, Liu J, Li K, Zhou Y, Huang H, Yang F. Do modic changes affect the fusion rate in spinal interbody fusion surgery? A systematic review and network meta-analysis. Journal of Clinical Neuroscience 2024;125:110–9. https://doi.org/10.1016/j.jocn.2024.05.019.
[7] Deng Y, Zhang X, Sheng X, Wang B, Hong Y, Rong X, Ding C, An J, Liu H. Modic Changes in Patients Who Have Undergone Anterior Cervical Discectomy and Fusion: The Correlation With Fusion Success and Subsidence. Orthop Surg 2025;17:1190–200. https://doi.org/10.1111/os.14377.
[8] Deng Y, Zhang X, Sheng X, Wang B, Hong Y, Rong X, Ding C, An J, Liu H. Modic Changes in Patients Who Have Undergone Anterior Cervical Discectomy and Fusion: The Correlation With Fusion Success and Subsidence. Orthop Surg 2025;17:1190–200. https://doi.org/10.1111/os.14377.
[9] Xiao Y, Xiu P, Yang X, Wang L, Li T, Gong Q, Liu L, Song Y. Does Preoperative Modic Changes Influence the Short‐term Fusion Rate of Single Level Transforaminal Lumbar Interbody Fusion?—a Matched‐pair Case Control Study. Orthop Surg 2023;15:2309–17. https://doi.org/10.1111/os.13795.
[10] Udby PM, Modic MT, Vestergaard T, Carreon LY. The Modic change grade is associated with patient-reported outcomes in lumbar spinal stenosis surgery. Clin Neurol Neurosurg 2025;257:109052. https://doi.org/10.1016/j.clineuro.2025.109052.
[11] Watanabe K, Fujii T, Michikawa T, Iga T, Okubo T, Takeda K, Suzuki S, Ozaki M, Tsuji O, Nagoshi N, Matsumoto M, Nakamura M. Ten-Year Clinical Outcomes After Decompression Surgery for Lumbar Spinal Stenosis: The Impact of Preoperative Modic Changes. Global Spine J 2026;16:918–27. https://doi.org/10.1177/21925682251361034.
[12] Heggli I, Mengis T, Laux CJ, Opitz L, Herger N, Menghini D, Schuepbach R, Farshad-Amacker NA, Brunner F, Fields AJ, Farshad M, Distler O, Dudli S. Low back pain patients with Modic type 1 changes exhibit distinct bacterial and non-bacterial subtypes. Osteoarthr Cartil Open 2024:100434. https://doi.org/https://doi.org/10.1016/j.ocarto.2024.100434.
[13] Heggli I, Laux CJ, Mengis T, Karol A, Cornaz F, Herger N, Aradi-Vegh B, Widmer J, Burkhard MD, Farshad-Amacker NA, Pfammatter S, Wolski WE, Brunner F, Distler O, Farshad M, Dudli S. Modic type 2 changes are fibroinflammatory changes with complement system involvement adjacent to degenerated vertebral endplates. JOR Spine 2023;6. https://doi.org/10.1002/jsp2.1237.
[14] Jensen TS, Karppinen J, Sorensen JS, Niinimäki J, Leboeuf-Yde C. Vertebral endplate signal changes (Modic change): A systematic literature review of prevalence and association with non-specific low back pain. European Spine Journal 2008. https://doi.org/10.1007/s00586-008-0770-2.