
The 71% Problem: When Spine Surgeons Disagree on the Same Patient — and Following Either Expert Doesn’t Help
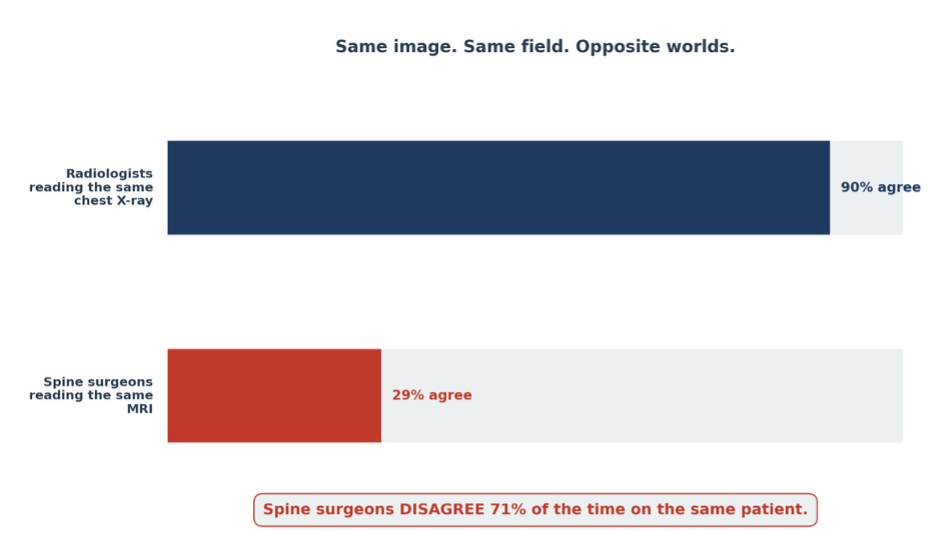
When five radiologists read the same chest X-ray for lung cancer, they agree 90% of the time. When five spines urgeons read the same MRI, they disagree 71% of the time. Same image. Same field. Opposite worlds. That gap is spine surgery’s unsolved problem.
But the harder finding is this:following the expert’s preference does not improve the outcome. The disagreement isn’t even productive. That changes how we should think about surgical decision-making — and what spine surgery actually needs to fix it.
The Disagreement Is Bigger Than You Think
In one study, 445 spine surgeons reviewed identical patient cases of lumbar spondylolisthesis [1]. They disagreed on which operation to perform 64% of the time when the patient had back pain, and 71% of the time when the patient did not. Two out of every three randomly chosen surgeons picked different operations for the same patient.
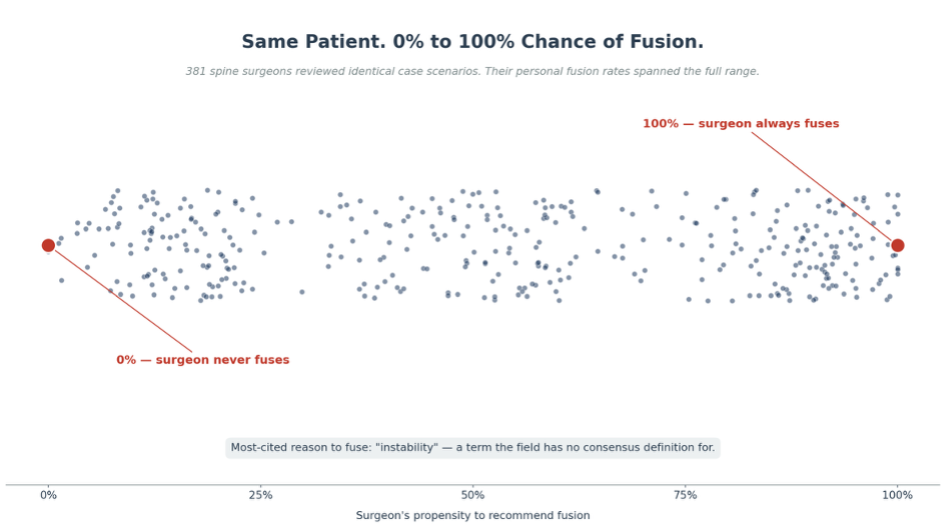
Morse and colleagues found the same pattern in a separate cohort of 381 surgeons [2]. For one-level degenerative spondylolisthesis, surgeons’ fusion rates ranged from 0% to 100% on identical case scenarios. The most common reason cited for fusing was “instability” — a term the field has no consensus definition for.
These are not edge cases or junior trainees. The data shows a counterintuitive pattern: more years of practice correlated with MORE disagreement, not less (70% disagreement among those practicing more than 20 years vs. 52% among those practicing 5 to 10 years). Specialty divides — orthopedic versus neurological surgery — added a second axis of variation (76% vs. 56% disagreement). The naive expectation is that experience converges on truth. The data shows the opposite. Variation is structural to the field, not a knowledge gap more training will close.
Same Trial. Same Eligibility Criteria. Different Operation.
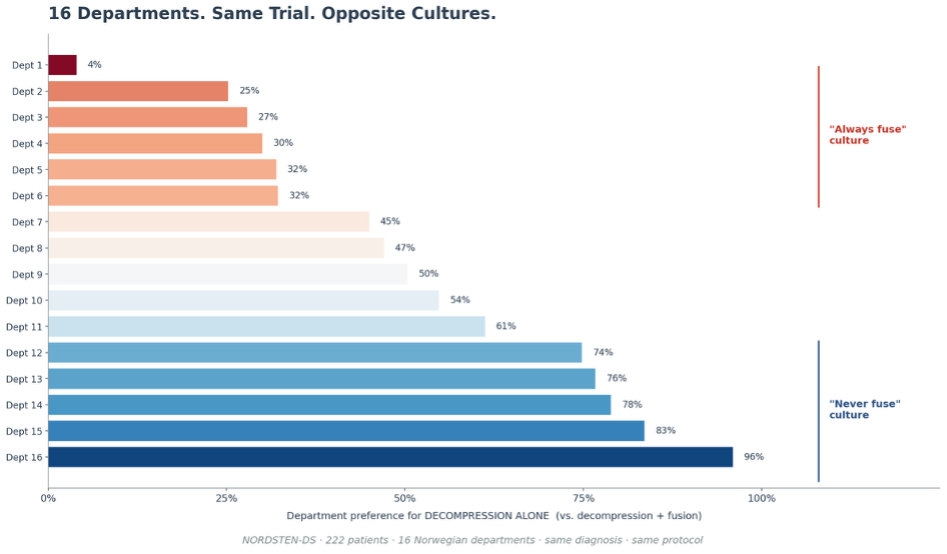
The most damning evidence comes from inside a randomized trial. The NORDSTEN-DS investigators ran a multi-center study of 222 patients with degenerative spondylolisthesis and stenosis across 16 Norwegian departments [3]. Same diagnosis. Same enrollment criteria. Same protocol. Before randomization, each operating surgeon recorded which procedure they would have preferred — decompression alone or decompression plus fusion.
Across the 16 departments, the preference for decompression alone ranged from near-zero to nearly 100%. Some departments were structurally “never fuse” cultures. Others were structurally “always fuse” cultures. They were treating the same kind of patient under the same trial.
The same pattern shows up at the population level. Deyo and colleagues analyzed 32,152 Medicare patients with lumbar stenosis only — no spondylolisthesis, no scoliosis [4]. Roughly one-third received fusion. Between 2002 and 2007, the total surgery rate barely changed (137 to 135 per 100,000 beneficiaries), but the procedure mix shifted entirely. Complex fusion procedures alone grew 15-fold (from 1.3 to 19.9 per 100,000). Same diagnosis code; three fundamentally different operations [5]. The variation is not noise. It is the system.
Following the Expert Doesn’t Help Either
NORDSTEN-DS randomized patients to decompression alone or decompression plus fusion regardless of the operating surgeon’s preference. At two years, the investigators compared outcomes for patients whose received procedure matched the surgeon’s prerandomization preference against patients whose procedure did not.
Of patients who got the procedure their surgeon recommended, 75% reached the primary outcome (a 30% or greater improvement on the Oswestry Disability Index). Of patients who got the OPPOSITE of what their surgeon recommended, 73% reached it. The difference was 2.4 percentage points, with a 95% confidence interval of −9.1 to +13.9. The interval crosses zero by a wide margin.
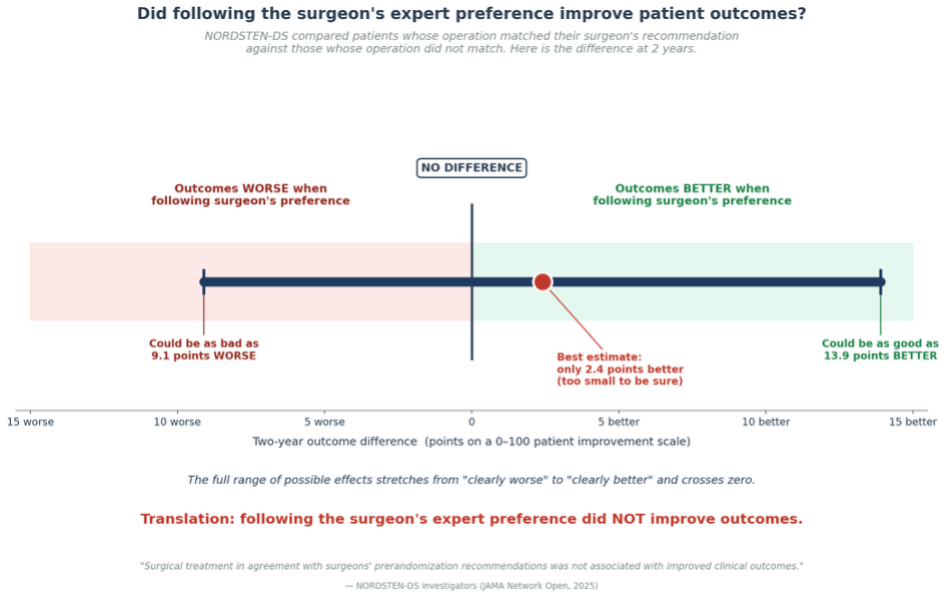
The finding is not that one procedure beat the other. It’s that following the operating surgeon’s expert opinion did not improve outcomes at two years. The disagreement was real. And it didn’t matter which expert was followed.
It’s Not the Patients. It’s the Evidence.
If there were a clearly superior operation for these patients, surgeons would converge on it. They have not. The simplest explanation is also the most likely: the patient-level evidence required to choose the right operation does not yet exist in a form a surgeon can act on at the bedside.
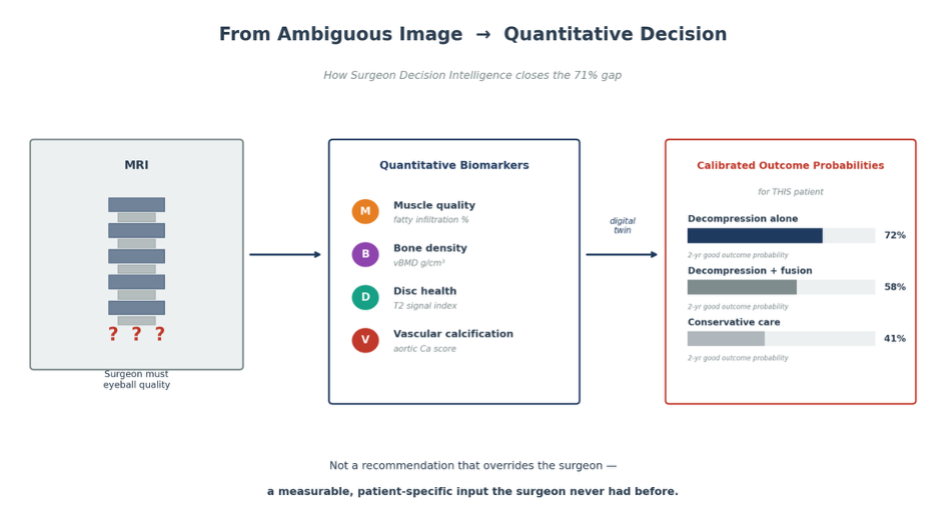
Spine surgeons have al ack of clarity. They work in a field where the key inputs — muscle quality, biomechanical reserve, vascular health, healing capacity — never get pulled out of the imaging as real numbers. The surgeon has to eyeball them.
This is the problem Surgeon Decision Intelligence is built to solve. Quantitative imaging biomarkers — muscle quality, disc health, vertebral bone density, vascular calcification — turn the inputs into measurable variables. A patient-specific digital twin compares surgical approaches against thousands of similar cases with two-year outcomes. The output is not a recommendation that overrides the surgeon. It is a calibrated probability of how each candidate operation is likely to perform for this specific patient. That’s the missing layer between 71% disagreement and clinical convergence.
The variation literature did its job. It proved the field cannot answer “which operation?” with today’s tools. The next decade decides whether we build the tools that can.
References
[1] Alentado VJ, Lubelski D, Williams SK, O’Rourke C, Obuchowski NA, Wang JC, Steinmetz MP, Melillo AJ, Benzel EC, Modic MT, Quencer R, Mroz TE. Variability in Surgical Treatment of Spondylolisthesis Among Spine Surgeons. World Neurosurgery. 2018 Mar;111:e564–e572. doi:10.1016/j.wneu.2017.12.108. PMID: 29288862.
[2] Morse KW, Steinhaus M, Bovonratwet P, Kazarian E, Gang CH, Vaishnav AS, Albert TJ, Iyer S, Qureshi SA. Current treatment and decision-making factors leading to fusion vs decompression for one-level degenerative spondylolisthesis: survey results from members of the Lumbar Spine Research Society and Society of Minimally Invasive Spine Surgery. The Spine Journal. 2022 Nov;22(11):1778–1787. doi:10.1016/j.spinee.2022.07.095. PMID: 35878759.
[3] Seip A, Hellum C, Fagerland MW, Solberg T, Brox JI, Storheim K, Hermansen E, Weber C, Brisby H, Banitalebi H, Furunes H, Indrekvam K, Ljøstad I, Austevoll IM. Surgeon Recommendation and Outcomes of Decompression With vs Without Fusion in Patients With Degenerative Spondylolisthesis. JAMA Network Open. 2025 Jan 2;8(1):e2453466. doi:10.1001/jamanetworkopen.2024.53466. PMID: 39777439.
[4] Deyo RA, Mirza SK, Martin BI, Kreuter W, Goodman DC, Jarvik JG. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA. 2010 Apr 7;303(13):1259–1265. doi:10.1001/jama.2010.338. PMID: 20371784.
[5] Birkmeyer JD, Reames BN, McCulloch P, Carr AJ, Campbell WB, Wennberg JE. Understanding of regional variation in the use of surgery. The Lancet. 2013 Sep 28;382(9898):1121–1129. doi:10.1016/S0140-6736(13)61215-5. PMID: 24075052.