
The Cost of Knowing Falls. The Cost of Caring Doesn't. Why AI Will Expand Healthcare Jobs.
Another apocalyptic AI memo hit my inbox last month. The Citrini Research scenario painted a familiar picture: by 2028, artificial intelligence triggers a global economic crisis. Unemployment goes from 2 to 10 percent. Mortgage markets collapse. Children go hungry as AI-driven productivity destroys the consumer economy.
What's striking isn't the memo. It's that this kind of thinking has gone mainstream. The logic feels airtight: AI replaces knowledge workers, workers lose income, demand falls, companies buy more AI to survive, and the cycle eats itself. Coders worry about Claude Code, analysts about Deep Research, SaaS companies about agents replacing them entirely. The professional class that built the knowledge economy is genuinely questioning whether knowledge work has a future.
But the narrative has a hole in it. It assumes every industry responds to AI the same way. They don't. Healthcare may be the industry where the doom case is most wrong, and the upside most underappreciated.
The History We Keep Forgetting
We have been here before. Every major technology looked like a job killer at first. Every single one ended up creating more work than it destroyed. Steam, electricity, computers, the internet - the pattern repeats so consistently that ignoring it requires deliberate effort.
Each wave moved labor up a layer rather than out of the economy. First it wiped out production labor - the direct task disappeared. Then it created coordination labor - managing the new systems became its own profession. Then it expanded meaning-and-experience labor: as survival got easier, people spent more on education, entertainment, and healthcare.
These transitions also took decades, not years. Steam took 40 years to fully reshape labor markets. Electricity took 40. Computers took 30. The internet took 25 [1]. Nobody woke up one morning and found a different economy. It was generational.
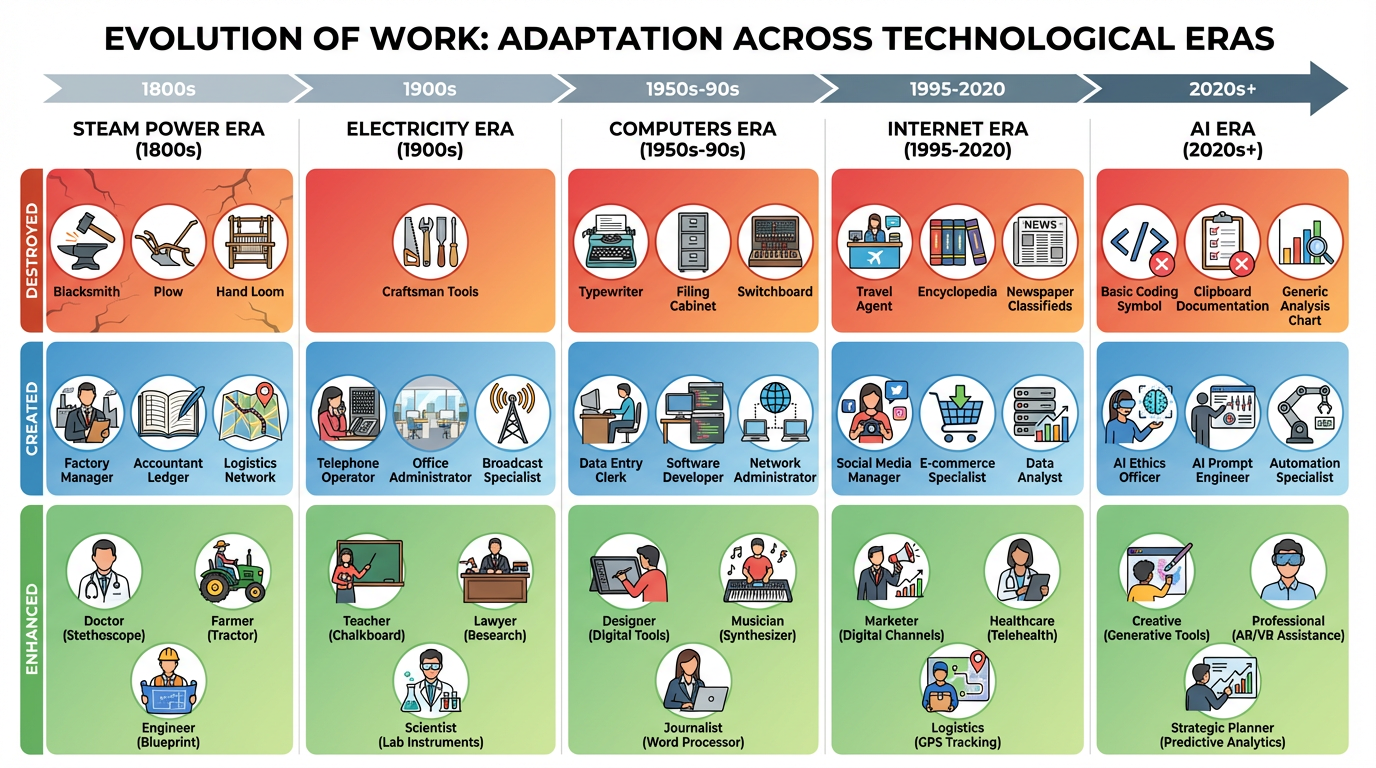
Each general-purpose technology compressed one layer of labor and expanded another. AI is the next iteration of that pattern.
AI is following the same arc. It automates routine cognition: coding, drafting, analysis, basic decisions. So humans move up another layer, from producing decisions to governing decision systems. The real question is which industries still need humans when intelligence becomes abundant.
Healthcare Operates by Different Rules
Most AI commentary assumes demand collapses when automation arrives. That assumption does not apply to healthcare.
Healthcare demand is income inelastic. People do not buy medical care because they feel wealthy. They buy it because biology fails. Heart attacks happen regardless of GDP. Joints degenerate on their own schedule. Aging continues through recessions and booms. Even in the worst economic scenarios, healthcare demand persists.
Medicine has always priced expertise, uncertainty, and decision confidence. Abundant intelligence reduces uncertainty. When diagnosis becomes cheap and reliable, value transfers from interpretation to intervention, and medicine transforms from a knowledge industry into an infrastructure industry.
This shift does not reduce healthcare spending. It increases it. When MRI scans became cheaper, imaging spending went up, not down — better scans found more treatable problems. When arthroscopy improved, orthopedic procedures expanded. When cardiac catheterization advanced, interventional cardiology exploded. Cheaper to know does not mean cheaper to treat.
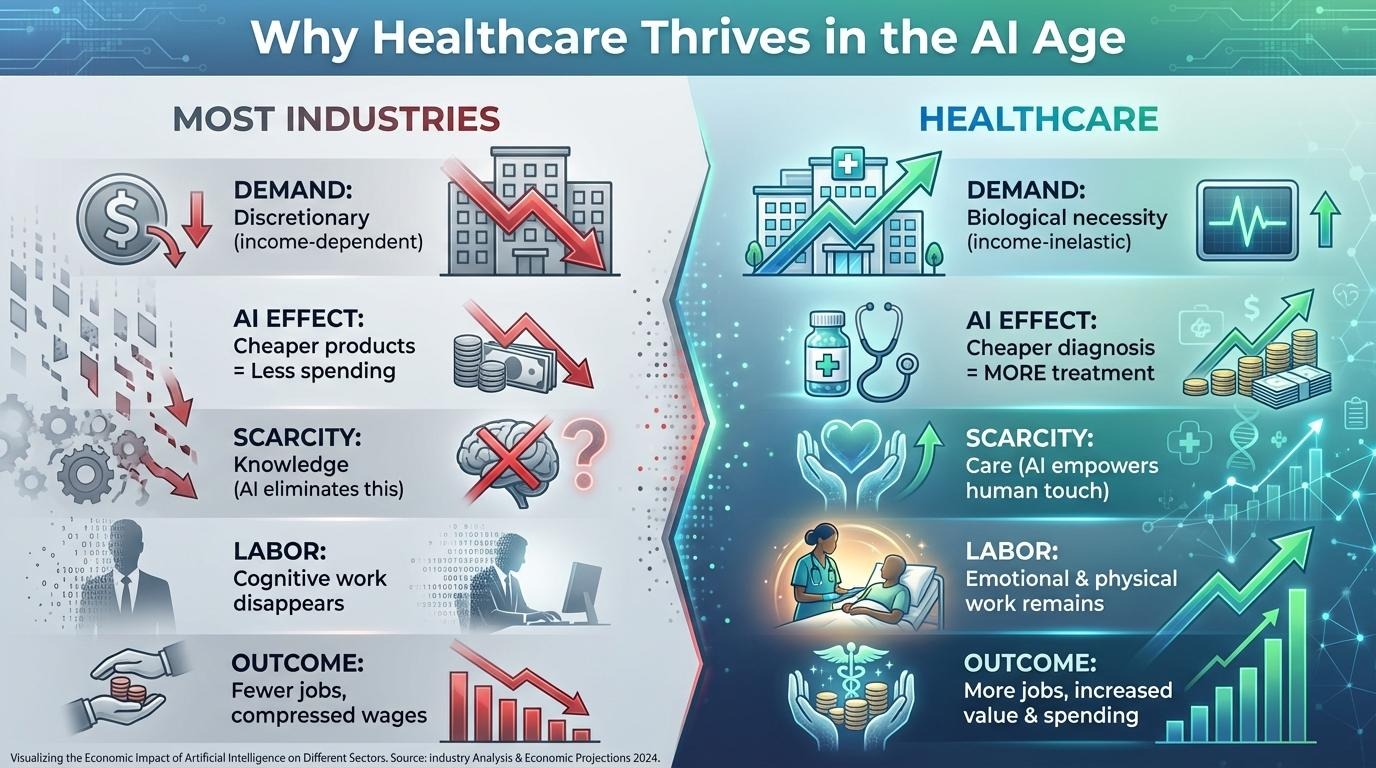
Healthcare's economic logic inverts the doom case: cheaper diagnosis expands eligibility, which expands volume, which expands hands-on labor.
The labor implications are concrete. AI removes documentation work, coding, basic radiology interpretation, and routine triage. It expands procedures, monitoring services, chronic disease management, and longevity care. Healthcare stops being primarily cognitive and becomes primarily hands-on, which makes the sector a natural absorber of workers displaced from cognition-heavy industries.
Why Surgery Sits in the Sweetest Spot
Surgery is the ultimate execution profession. It converts knowledge into physical change. And right now, surgeons spend enormous time and energy on something AI is genuinely good at: deciding whether and which intervention is necessary.
That decision-making currently dominates patient visits, peer discussions, and conferences. AI will compress most of the uncertainty out of it. Models trained on tens of thousands of cases will predict surgical outcomes with accuracy no individual surgeon can carry in their head. The question shifts from whether surgery helps to when it should happen. That doesn't reduce surgical volume - it increases it. Ideally with fewer inappropriate procedures and many more appropriate ones.
Spine surgery is the textbook case. It is imaging-intensive, aging-driven, and deeply affected by exactly the kind of diagnostic uncertainty AI can resolve. Quantitative imaging biomarkers extracted from MRI - muscle quality, disc health, vertebral bone density, vascular calcification - are moving the field from subjective grading to continuous, objective measurement. Layered with patient-specific simulation, they predict not just if surgery helps but which approach gives this individual the best two-year functional outcome. This is the shape of what we are building at Surgeon Decision Intelligence: tissue-typing biomarkers feeding a digital twin that compares surgical approaches before the incision. When uncertainty falls, candidacy rises. More patients qualify for treatment when you can actually predict who benefits.
What the New Jobs Actually Look Like
There are more new healthcare jobs in an AI-enriched world than the doom narrative imagines. Clinical AI governance alone is enormous. Healthcare cannot run on autonomous decisions without human accountability. AI safety auditors, algorithm validation physicians, and model-risk specialists who navigate liability when AI-assisted decisions cause harm aren't speculative roles. Healthcare is 18 percent of US GDP. If just 3 percent of healthcare workers shift into AI oversight, that's roughly 500,000 new positions, all of them requiring medical training and regulatory expertise.
Pre-op optimization is the bucket nobody is talking about yet. Once AI can tell a surgeon this patient will most optimally benefit from L4-L5 fusion only if they do prehab for 3 months, lose a certain amount of weight, and quit nicotine, somebody has to actually deliver that optimization. Surgical prehabilitation physical therapists, nutrition coaches gating elective surgery, smoking-cessation counselors, sleep-hygiene clinicians. These aren't new categories of work — they exist today in narrow corners. They become standard infrastructure the moment an algorithm can identify in advance which patients turn into successful operations only after eight weeks of preparation. AI doesn't shrink the workforce around a surgical episode. It expands it backward in time.
Continuous monitoring expands dramatically as medicine shifts from episodic care to persistent modeling. Patient trajectory managers overseeing AI systems that simulate disease progression. Remote recovery analysts tracking post-surgical healing through wearables, gait sensors, and digital outcome metrics that replace the once-quarterly questionnaire. Predictive care planners intervening before deterioration becomes acute. A fundamentally different labor profile than today's healthcare workforce.
Procedural expansion is larger than the OR itself. More patients qualifying for surgery means more of every role that touches a surgical episode. Inside the OR: more surgeons doing more cases, anesthesiologists and CRNAs scaling with volume, robotics operators and interventional technologists running new platforms, perioperative nurses, scrub techs, PACU staff. After the case: physical therapists, occupational therapists, home health nurses, recovery coaches — already among the fastest-growing occupations of the next decade per BLS projections [3], and growing further the moment surgical volume rises. Each intervention has a long tail of human hands attached to it.
The Cost of Knowing vs. the Cost of Caring
The fear is that AI removes work because machines produce everything. The reality is that AI removes the cost of knowing, but not the cost of caring. Industries built on knowledge will shrink. Industries built on biology will expand. Surgical care sits at the intersection of human trust and physical intervention, and both remain scarce even when intelligence is abundant.
It's worth grounding this in something concrete. The World Economic Forum projects AI will create roughly 97 million new jobs by 2025 against 86 million displaced [2]. The number gets mocked, but it bottoms out in three real mechanisms: role expansion in existing occupations, hybrid jobs that didn't have titles five years ago, and the classical induced-demand effect — automation raises productivity, prices fall, real incomes rise, and people spend the surplus on what remains scarce. The WEF model doesn't fully account for that third channel. Which means 97 million is probably an undercount. And healthcare may be the largest beneficiary of all of it.
References
[1] Brynjolfsson E, Rock D, Syverson C. The Productivity J-Curve: How Intangibles Complement General Purpose Technologies. American Economic Journal: Macroeconomics. 2021;13(1):333–372.
[2] World Economic Forum. The Future of Jobs Report 2020. Geneva: World Economic Forum, 2020.
[3] U.S. Bureau of Labor Statistics. Occupational Outlook Handbook: Healthcare Occupations. Home health and personal care aides, physical therapist assistants, occupational therapy assistants, and registered nurses all rank in the top tier of projected job growth for 2022–2032.