
The Spine Fellowship of 2030: What Changes When the Trainee Has Decision Intelligence on Day One
Ask any senior spine surgeon what is hardest about training a fellow, and they won't tell you about techniquee. They'll tell you about the decision. The technical work (the access, the instrumentation, the closure) is teachable in a couple hundred cases. Knowing which patient should have the operation in the first place takes a career. Every generation of surgeons has rediscovered some version of the same surgical aphorism: any fool can cut; it takes a long time to learn when not to.
I think about this with new fellows. They will graduate with technically sound hands long before they graduate with calibrated judgment. The gap between those two competencies is the most important thing surgical training does not have a good answer for. I think AI may finally provide one. And that the fellow walking into our operating room in 2030 will be a fundamentally different trainee than the one I was.
The Pattern-Recognition Bottleneck
Surgical training has always been an apprenticeship of accumulated cases. Fellows this year will log somewhere around 300 cases (recent ACGME-derived benchmarks put the mean at 322 [1]). Their judgment will then be calibrated by the next thousand cases over the following decade. Many of those they will get wrong before they get them right.
This is the central bottleneck of how we train surgeons. Pattern recognition is built one case at a time, and the early cases pay the cost. The senior surgeon's wisdom — the part of practice that takes a career — comes from cases the fellow has not yet seen and won't see for years. Pattern memory cannot be transferred through words or video alone. It has to be experienced to some degree.
What changes in 2030 is not the volume of cases the fellow performs. They will still operate roughly 300 times in fellowship. What changes is the volume of cases they can learn from. The fellow's pattern-recognition base is no longer bounded by the cases at their institution.
What 'Decision Intelligence on Day One' Actually Means
Decision intelligence in this context does not mean a black box that issues a recommendation. It means fellows open a case with structured access to outcome patterns from tens of thousands of similar cases — calibrated probabilities for each surgical approach, the variables that drive those probabilities, and an honest signal of where the model is uncertain.
From where I sit at the head of the table, this shifts the daily learning in three concrete ways.
First, the fellow can sanity-check intuition against evidence in the moment. Their gut says ALIF. The model puts ALIF third behind a hybrid approach. Now attendings are not just listening to them articulate a plan — they arelistening to them articulate why their gut disagrees with thousands of similar cases. That articulation is itself a learning event our generation rarely had to perform.
Second, the fellow starts asking better questions during the case. "The model flags a 40 percent reoperation risk for this approach in patients with this paraspinal muscle profile. What would change your plan?" That question forces attendings into a different kind of teaching. Less demonstration, more explicit reasoning
Third, the fellow learns calibration explicitly. When the model is uncertain, the fellow learns that uncertainty is the right response, not bravado. This is the subtlest and most valuable shift. Surgical culture has historically rewarded certainty. Calibration teaches a different relationship with confidence — one where saying "I don't know, the data is thin here" is a sign of skill and nuance.
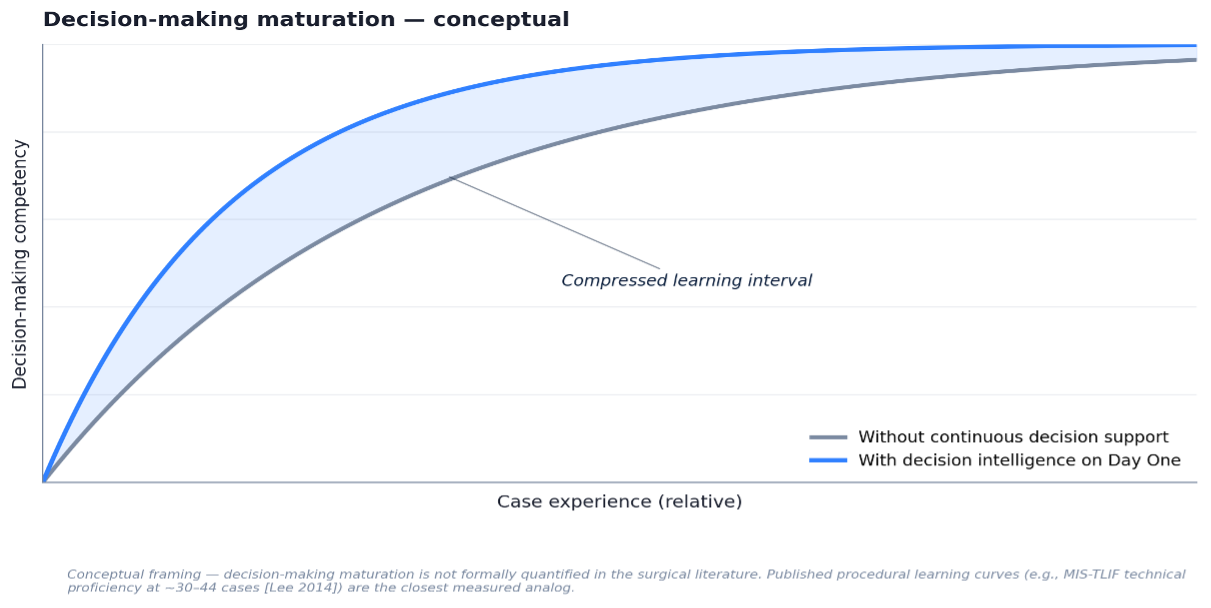
A note on what is and is not measured here. Procedural learning curves are measured carefully — technical proficiency for MIS-TLIF, for instance, is typically reached around 30 to 44 cases [2]. Decision-making maturation is harder to quantify, and to our knowledge no published study has measured it directly. The curves above are conceptual rather than fitted to data, and the empirical question of whether decision intelligence actually compresses the interval is exactly what the next decade should answer.
What This Changes About Mentorship
The reflexive worry I hear from colleagues is that decision intelligence will weaken trainees. If the algorithm is doing the thinking, the fellow never has to. The reasoning sounds plausible. It does not survive contact with what actually happens in operating rooms that have adopted decision support tools in adjacent specialties.
The closest analog is anesthesiology in the 1980s, when pulse oximetry moved from novel to standard of care. The same fear came up — if anesthesiologists rely on the monitor, will they lose physical exam skills? They did not. What happened instead was that pulse oximetry freed cognitive bandwidth from one task, and that bandwidth went into harder problems the previous generation never had time to think about. The standard of care rose. So did the ceiling of what anesthesiologists could attend to.
Decision intelligence does the same thing for fellows. It does not replace judgment. It externalizes one specific, narrow part of judgment — pattern recall across thousands of similar cases — so the fellow's cognitive bandwidth can go elsewhere.
What changes about mentorship is the level of abstraction. Teachers spend less time saying "let me show you what I have seen" and more time saying "let me show you when to override the model and why." That is mentorship at a higher altitude — about judgment under uncertainty rather than rote technique. It is also the kind of mentorship that those of us teaching surgical fellows have always wanted to give and rarely had the time for.
The Path Forward
The first cohort of fellows trained this way will graduate within the decade. Those of us who run programs and adopt decision intelligence early will be in a position to study what changes — does autonomy come faster, do early errors decrease, do our trained surgeons carry better calibration into independent practice. These are answerable questions. They have not been answerable before because the comparator did not exist.
Surgical training has always been an apprenticeship of accumulated cases. Decision intelligence does not break that model. It gives every apprentice access to the accumulated cases of thousands of mentors at once. The fellowship of 2030 will not replace the master surgeon. It will produce one faster — and it will produce one with the kind of calibration the senior surgeons I trained under always taught but rarely had the data to measure.
References
[1] Daniels AH, Reid DBC, Durand WM, et al. Establishing case volume benchmarks for ACGME-accredited orthopedic surgery of the spine fellowship training. Spine J. 2024;24(8):1490–1497.
[2] Lee KH, Yue WM, Yeo W, Soeharno H, Tan SB. Clinical and radiological outcomes of open versus minimally invasive transforaminal lumbar interbody fusion. Eur Spine J. 2012;21(11):2265–2270. See also: Lee JC, Jang HD, Shin BJ. Learning curve and clinical outcomes of minimally invasive transforaminal lumbar interbody fusion. Spine. 2012;37(18):1548–1557 — describes technical proficiency at ~30 cases.