
The Big Data Promise That Never Came to Healthcare
We were promised a revolution. Ten years ago, tech conferences buzzed with excitement about artificial intelligence and machine learning transforming medicine. Algorithms would crunch massive datasets and tell us exactly which treatment works best for which patient. Personalized medicine would become the standard. Doctors would make better decisions, faster.
So where is it?
If you're a spine surgeon in 2026, you're not experiencing arevolution. You're experiencing decision paralysis.
The Explosion of Surgical Options
Consider what a spine surgeon faces today when treating a patient with back pain and radiculopathy. The image below captures this perfectly: The Spine Surgery Decision Paradox.
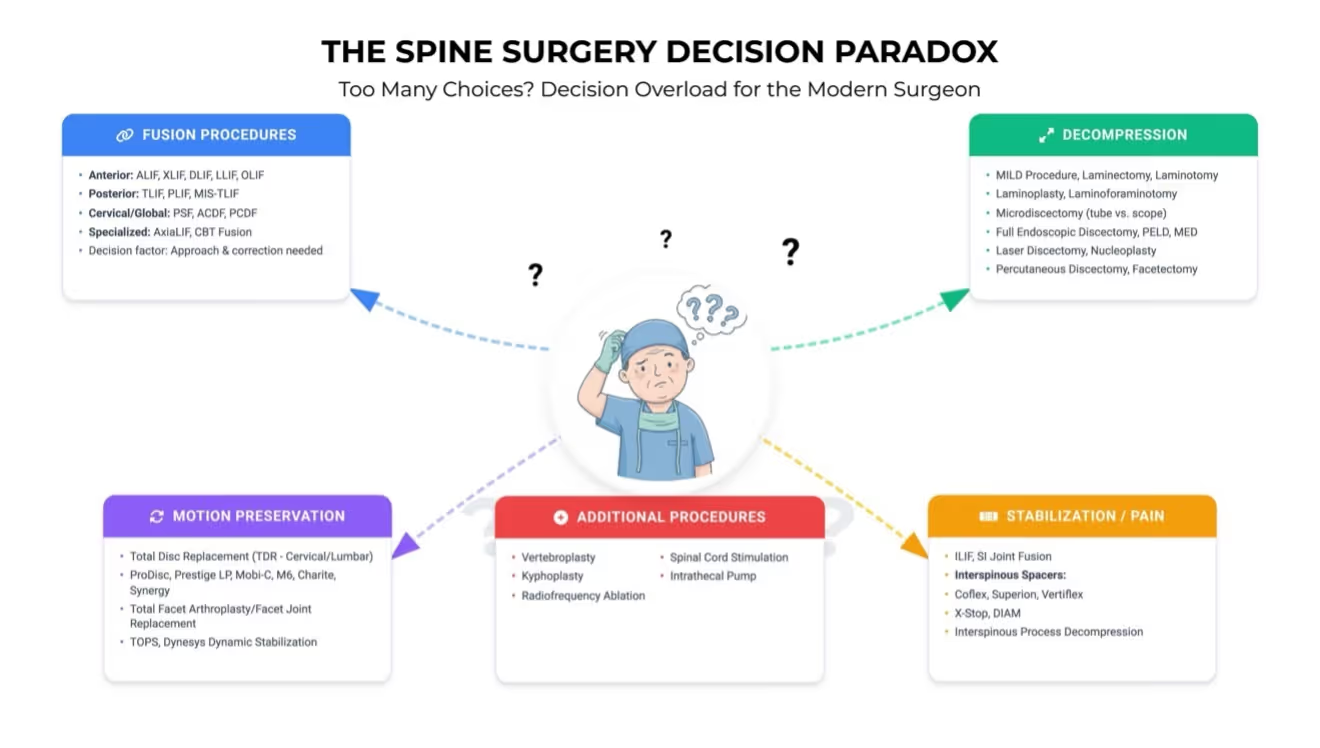
Just within fusion procedures alone, surgeons must choose between anterior approaches like ALIF, XLIF, OLIF, and LLIF, or posterior approaches like TLIF, PLIF, and MIS-TLIF. Cervical cases add PSF, ACDF, andPCDF to the mix. And that's just fusion—one category among dozens. Add decompression procedures, motion preservation techniques, pain management interventions, and stabilization options, and you have over 40 distinct surgical approaches for spine pathology. Each procedure comes with its own learning curve, cost considerations, and manufacturer claims about superior outcomes. We are drowning in choices.
The Information Overload Crisis
Modern spine surgeons don't suffer from a lack of options.They suffer from too many options with too little guidance about which one actually works best for the patient sitting in front of them.
Every implant company claims their device is revolutionary.Every new surgical technique promises better outcomes with fewer complications.Sales representatives schedule lunches to show impressive-looking charts.Journal articles funded by device manufacturers tout marginal improvements in surrogate endpoints.
But when you have a 52-year-old construction worker withL4-L5 degenerative disc disease, moderate stenosis, and a 20-year smoking history sitting in your office, which procedure actually gives him the best chance of returning to work pain-free?
You don't know. Nobody knows. And that's the problem.
The AI Promise: What Happened?
This is exactly the problem artificial intelligence and machine learning were supposed to solve. Feed the algorithms thousands of patient cases with detailed outcomes data, and they'd identify patterns invisible to human eyes. They'd tell you that patients with this specific combination of imaging findings, demographics, and clinical symptoms do best with that specific procedure.
Netflix can predict which movies you'll like based on your viewing history. Amazon knows what you'll buy before you know you need it. Your smartphone suggests restaurants based on your location and eating habits.
Why can't we get an algorithm to suggest the right spine surgery for the right patient?
The Missing Ingredient: Quality Data
The answer is brutally simple: garbage in, garbage out.
AI needs data—lots of it—and it needs good data. Healthcare has plenty of data, but most of it is terrible for training algorithms.
Medical records are fragmented across different electronic health systems that don't talk to each other. Imaging studies sit in isolatedPACS systems. Follow-up is inconsistent. When patients get surgery at one hospital and follow-up care at another, outcomes data disappears into the void.
Even when data exists, it's biased. Device manufacturers fund studies of their own products, creating selection bias. Surgeons preferentially use certain techniques for certain patient types, creating confounding. Negative results don't get published, creating publication bias.
Most critically, comprehensive datasets simply don't exist.You might have operative reports without preoperative imaging. Or MRIs without long-term follow-up. Or outcomes data without information about surgical technique. Trying to train an AI on incomplete, biased, fragmented data is like trying to teach someone to cook by showing them random ingredients without recipes.
Collaboration between institutions is rare. Data sharing faces regulatory hurdles, privacy concerns, and competitive pressures. So each hospital, each surgeon, each research group works in isolation with their own small, incomplete dataset.
A Different Approach: The Surgeon Decision Intelligence (SDI) System
This is what makes the SDI System's foundational model genuinely unique.

The numbers tell the story: 100,000 spine MRIs with comprehensive imaging data. 50,000 operative reports with detailed surgical technique documentation. And here's the critical part: 90% two-year follow-up with longitudinal patient tracking.
This isn't just one type of data. It's multi-modal data—X-rays, CT scans, and MRIs for the same patients.Clinical information, surgical details, and long-term outcomes all linked together in a centralized hub for advanced analytics.
This type of comprehensive dataset is unheard of in theUnited States. Most research studies follow a few hundred patients for a few months. Device company registries capture thousands of cases but lack detailed imaging or independent outcome verification. Academic institutions have detailed data on their own patients but can't scale.
SDI has built something different: the foundation for actually training AI that can guide surgical decision-making.
The Right Surgery for the Right Patient
With quality data, AI can finally deliver on its promise.Imagine inputting your patient's complete clinical picture—demographics, imaging findings, symptoms, comorbidities, smoking status, occupation—and receiving evidence-based guidance about which procedure offers the best functional outcome versus the best durability versus the best overall match.
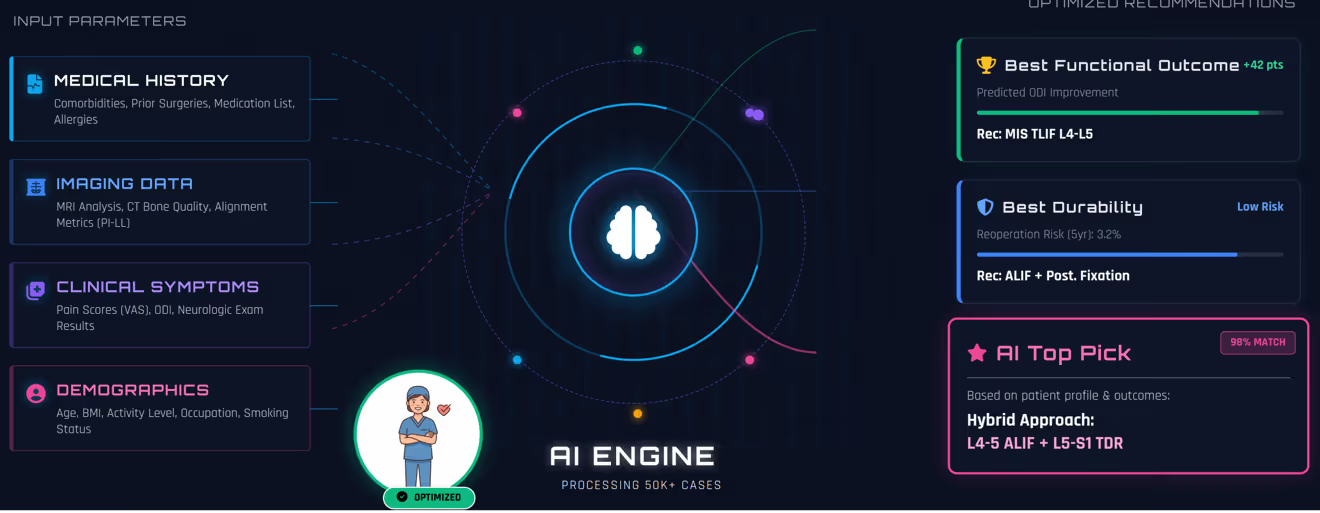
This isn't science fiction. The image above shows what this could look like in practice. The AI processes comprehensive patient data and generates optimized recommendations based on 50,000+ similar cases. For that52-year-old construction worker, it might show that MIS TLIF at L4-L5 offers the best outcome in terms of return to physical function. ALIF with posterior fixation provides the lowest reoperation risk at 3.2% over five years for best durability. But the top pick, with a 98% match based on his specific profile, might be a hybrid approach: L4-5 ALIF plus L5-S1 TDR.
These aren't marketing claims from an implant company. These are data-driven insights from thousands of real patients with similar characteristics and long-term follow-up.
This is what "the right surgery for the right patient" actually means. Not intuition. Not the procedure you trained on.Not the device the sales rep promoted last week. Evidence-based, individualized recommendations grounded in comprehensive outcomes data.
Conclusion: The Day May Finally Come
For years, we've heard promises about big data and artificial intelligence revolutionizing healthcare. We've been wondering why the revolution never arrived.
Now we know: it was the data all along. You can't build transformative AI on fragmented, biased, incomplete information any more than you can build a skyscraper on quicksand.
But when you have 100,000 spine MRIs with 90% two-year follow-up and comprehensive multi-modal imaging? When you have 50,000 operative reports linked to clinical outcomes? When you build a foundational model on quality data instead of garbage?
That's when the revolution becomes possible.
The algorithm that tells us what to do—the one we've been promised for a decade—may finally be within reach. The day when we confidently recommend the optimal procedure for each individual patient, backed by evidence from thousands of similar cases, might actually come.
For spine surgeons drowning in choices and patients desperate for answers, that day can't come soon enough.